MeetYourClinic Editorial Team
Medical Tourism Research · Updated Feb 2026
Quick Summary
FUE and DHI are often presented as competing hair transplant ‘methods’, but the real difference is usually how grafts are implanted. This guide explains what changes, what it costs in the UK vs Turkey, and how to choose safely.
If you are comparing FUE and DHI hair transplants, you are already asking the right question: what actually changes in the operating theatre, and does it change your result?
Both methods usually use FUE harvesting (taking follicular units one by one with a small punch) and then differ mainly in how the grafts are implanted. DHI is not a separate “type of hair” that is implanted, and it is not automatically “better”. It is a tool-and-workflow choice that suits some cases and some surgical teams.
This 2026 guide explains the practical differences, the real-world cost gap (UK and Turkey), who each approach tends to suit, and the red flags to avoid.
Quick Summary (snippet-ready)
- FUE vs DHI is mostly an implantation difference. In many clinics, both start with FUE harvesting, then FUE uses pre-made recipient sites (channels) before placing grafts, while DHI places grafts using an implanter pen that creates the site and inserts the graft in one step.[1–3]
- Results depend more on the team than the label. Hairline design, donor management, graft handling (time out of body, hydration, temperature), and who does each step matter more than whether a pen was used.[1,4]
- DHI often costs more because it can be slower, more staff-intensive, and uses single-use pen/needle systems. It can be useful for small areas, touch-ups, and some no-shave cases, but it is not automatically higher density.
- Sapphire FUE usually means sapphire blades were used to create recipient sites. It is a variation within “FUE-style implantation”, not a separate harvest method, and evidence of meaningful superiority is limited.[3]
- Choose a clinic by process and accountability, not marketing. You should know exactly who is designing the hairline, who is doing extraction and implantation, what the daily graft cap is, and what happens if you need follow-up.
Definitions in plain English
What “FUE” actually means
Follicular Unit Extraction (FUE) is a way of harvesting grafts. Individual follicular units are removed from the donor area using a small punch (often around 1 mm), rather than removing a strip of scalp (FUT/strip).[1]
FUE is popular partly because it leaves many tiny dot scars instead of a linear scar, but it still requires skill. Over-harvesting can visibly thin the donor area.[4]
What “DHI” actually means
Direct Hair Implantation (DHI) is usually a way of implanting grafts. The graft is loaded into an implanter pen (pen-like device with a hollow needle), and the pen is used to create the recipient site and place the graft in one motion.[2]
Many clinics advertise “DHI” as if it is separate from FUE, but in practice, harvesting is very often still performed with FUE. Think of DHI as “FUE harvesting + pen implantation”.
What “Sapphire FUE” actually means
“Sapphire FUE” typically refers to using a sapphire blade to create recipient sites (channels) for graft placement. It is still usually FUE harvesting, with a particular material used for incisions during site creation.[3]
FUE vs DHI vs Sapphire FUE: side-by-side comparison
| Feature | FUE (standard implantation) | DHI (implanter pen) | Sapphire FUE (channel blades) |
|---|---|---|---|
| Harvest method | Usually FUE punch extraction[1] | Usually FUE punch extraction[1] | Usually FUE punch extraction[1] |
| How recipient sites are made | Channels made first, then grafts placed | Site is created and graft is inserted with the pen[2] | Channels made first using sapphire blades[3] |
| Speed for large sessions | Often faster for big cases | Can be slower because each placement is “one-by-one” with the pen | Similar to standard channel method |
| Shaving / no-shave friendliness | Both possible, depends on technique and graft numbers | Often marketed for no-shave or partial shave, but case-dependent | Case-dependent |
| Density claims | High density is possible, but limited by scalp blood supply and safe packing | Often marketed as “higher density”, but not guaranteed | Often marketed as “finer incisions”; outcomes depend more on the surgeon |
| Typical cost (UK/Turkey) | Usually lower than DHI | Often higher than standard FUE | Often similar to, or slightly higher than, standard FUE |
| Best suited for (typical) | Most first-time cases, larger areas, budget control | Smaller areas, touch-ups, some no-shave cases, teams experienced with pens | Patients choosing a channel method where the surgeon prefers sapphire blades |
Note: Terms are used inconsistently. Always ask for the step-by-step plan for your case rather than relying on the label.
The differences that actually affect results
1) Hairline design and planning
A natural hairline is about angles, irregularity, and appropriate density, not just graft count. The surgeon should plan:
- where density matters most (usually the frontal third)
- how to handle existing miniaturised hairs
- how the design fits future loss (so it does not look “too low” later)
No implantation tool can rescue a poor plan.
2) Donor management (the part you cannot replace)
Your donor area is finite. In FUE, extraction pattern and spacing matter, and over-harvesting increases the risk of visible thinning.[4]
Good clinics will talk to you about:
- realistic graft yield for your hair calibre and donor density
- avoiding “mega sessions” that look attractive on a quote but stress the donor
- long-term strategy if you may progress to higher Norwood patterns
3) Graft survival basics: handling, hydration, and time
The biology does not care whether the graft is placed with forceps or a pen. Survival depends on careful handling (avoiding crush injury), keeping grafts hydrated, and minimising time out of the body. This is one reason team training and workflow matter so much.
4) Recipient site creation and angle control
Both methods can produce excellent angle control. In channel-first approaches, the surgeon sets the angles and directions during site creation; in pen-based approaches, angle control happens as the pen inserts the graft.
In experienced hands, both can be precise. In inexperienced hands, both can be messy.
Costs in 2026: what you will typically pay (UK and Turkey)
Hair transplant pricing is messy because some clinics quote per graft, others quote per day, and many Turkey packages quote all-inclusive (hotel, transfers, translator) with a broad graft range.
Below are practical ranges you will commonly see in 2026 for reputable clinics. They are not promises, and you should judge value by the process, not just the number.
Typical price ranges (rule-of-thumb)
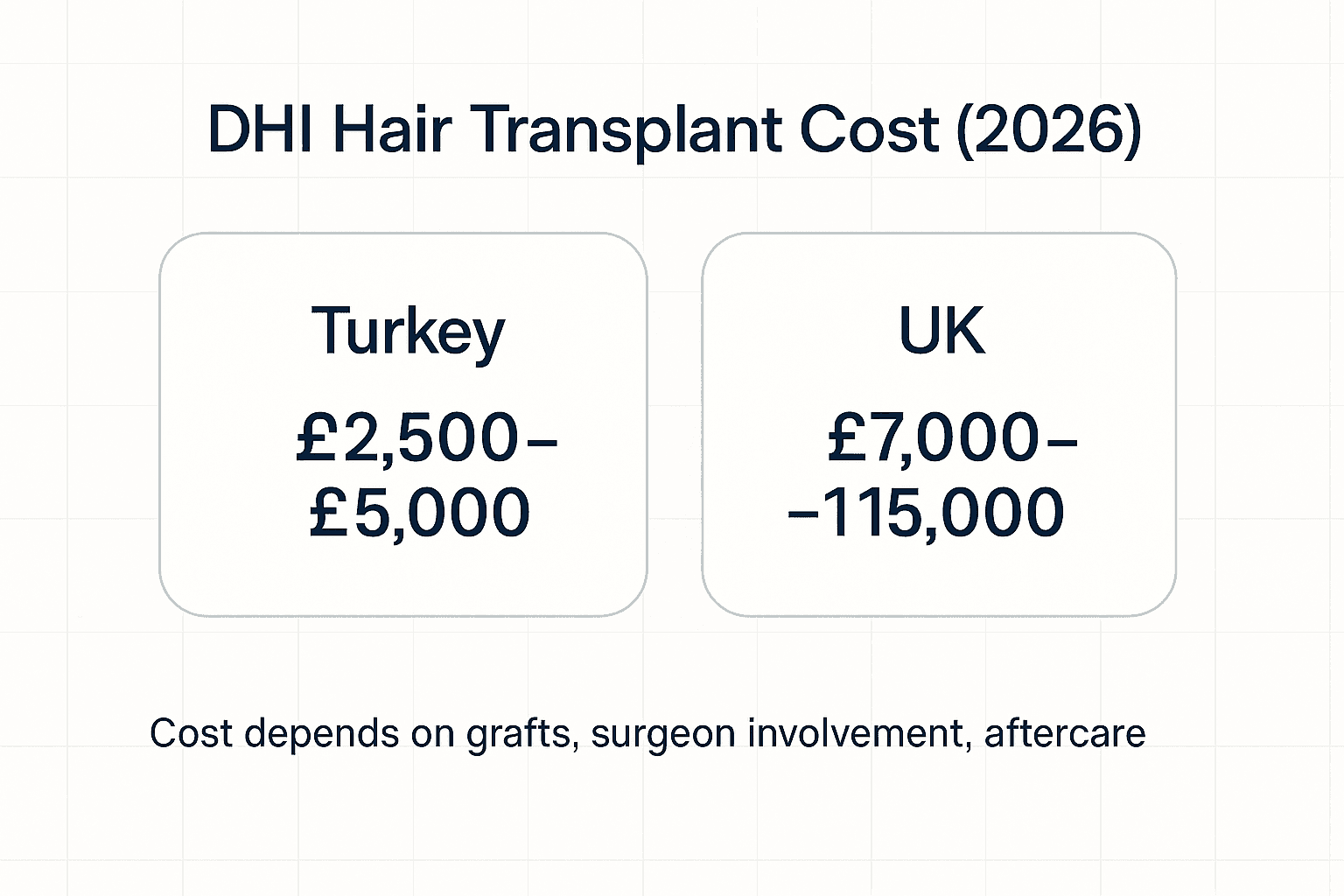
- UK (reputable, surgeon-led): often £4,000 to £12,000+ depending on graft numbers, surgeon time, and whether it is a complex repair case. Per-graft pricing is commonly used.
- Turkey (reputable, surgeon-led clinics): often £2,000 to £6,000 for many straightforward cases, with higher prices for clinics where the surgeon is highly involved, uses smaller daily graft caps, or focuses on repairs.
Why DHI is often more expensive
Even when the harvest is the same (FUE), DHI can cost more because:
- Time and staffing: loading pens and placing grafts one-by-one can be slower and more labour-intensive.
- Consumables: implanter pens and needles add per-case consumable costs.
- Training and consistency: good pen work needs a well-drilled team. Clinics that do it well often limit daily graft numbers.
Why UK prices are usually higher than Turkey
The gap is not automatically about quality. It often reflects:
- higher staff costs, insurance, and facility overheads
- stronger regulatory expectations and documentation
- the opportunity cost of surgeon time (especially if the surgeon does most steps)
The trade-off is that in the UK you may find it easier to verify clinician registration, regulation, and redress routes if something goes wrong.
A more useful way to compare: cost per surviving graft
A cheaper quote can be false economy if graft survival is poor, the hairline is wrongly designed, or the donor is over-harvested and you later need repair work.
When comparing quotes, ask:
- how many grafts they expect you need (and why)
- who is doing the extraction and implantation
- what their daily graft cap is
- what their plan is if your growth is below expectation at 12–18 months
Internal reading: Hair transplant cost (2026), Hair transplant cost in the UK (2026), and Hair transplant in Turkey guide.
Ready to Compare Clinics?
Get verified quotes from top-rated procedures clinics. Compare prices and reviews in minutes.
Who FUE is best for (in practice)
FUE with channel-first implantation is a workhorse approach and suits a wide range of patients, particularly:
- first-time patients needing frontal third restoration
- larger areas where efficiency matters
- people who prioritise predictable workflow and want the surgeon to set recipient-site angles up front
- patients who do not need a strict no-shave plan
Shave vs no-shave (FUE)
“Unshaven FUE” and “partial shave” options exist, but they add complexity and time. For bigger sessions, a full shave is often recommended because it can reduce transection risk and improve graft handling.
Who DHI is best for (in practice)
DHI (pen implantation) can be a good fit when the clinical goal is very specific and the team is genuinely experienced with pens. It is often considered for:
- small-to-medium areas (hairline refinement, temples, crown touch-ups)
- some no-shave or partial shave cases (especially when graft numbers are modest)
- patients who already have hair and want to work between existing hairs (this is case-dependent)
The “density” myth
DHI is often marketed as higher density because the pen creates and implants in one step. In reality, density is limited by scalp blood supply and safe packing. High density is possible with both workflows, but it depends on planning and technique, not branding.
When DHI may be a poor fit
DHI can be less attractive if:
- you need a very large graft number in one session and the clinic’s workflow becomes rushed
- the clinic is selling “DHI” but cannot explain who implants, what pen sizes are used, or how they protect grafts from dehydration
Recovery, scarring and timelines (what to expect)
Most patients experience some swelling, scabbing, and redness. The timelines are broadly similar across FUE and DHI because the biology is the same.
The usual timeline (very general)
- Days 1–3: swelling is common (especially forehead), donor area can feel tight/sore.
- Days 4–14: scabs form and then shed. Redness may persist longer in fair skin.
- Weeks 2–8: shedding of transplanted hairs is common (“shock loss”).
- Months 3–6: early growth.
- Months 9–12: more mature growth.
- 12–18 months: final maturation, especially in the crown.
Scarring
- FUE harvesting leaves small dot scars. Punch size, extraction pattern, and healing vary by patient.[1,4]
- DHI does not eliminate donor scarring because harvesting is often still FUE.
“Shock loss” and existing hair
Shock loss can affect existing miniaturised hairs around the transplanted area. This is one reason some clinics discuss medical therapy (for example, finasteride or minoxidil) as part of a long-term plan, where appropriate and medically suitable.
Red flags (UK and Turkey) to take seriously
These are the patterns we see repeatedly in unhappy outcomes and repair cases.[4]
- You cannot speak to the surgeon until the day of surgery. Planning is not a “sales call”.
- The clinic will not name who does extraction and implantation. If a technician does most steps, that should be explicitly stated.
- Unlimited graft promises (for example “5,000 grafts for everyone”) without assessing donor capacity.
- Heavy discounts for booking immediately or “deposit today” pressure.
- No discussion of future hair loss (only today’s hairline).
- No clear complication plan (infection, necrosis, poor growth, excessive scarring).
- Photo-only follow-up with no option for clinical review if you have concerns.
Clinic selection: questions to ask (copy/paste)
About the surgeon and team
- Who will design my hairline and make the medical plan?
- Who performs the FUE extractions?
- Who performs implantation (and what percentage does the surgeon do)?
- How many transplants does the team perform per day?
About technique choices
- Why are you recommending FUE vs DHI for my case?
- If DHI: which pen system do you use, and what needle sizes?
- If channel-first: what blades/needles do you use for recipient sites (steel vs sapphire), and why?
About donor safety and graft numbers
- What is my estimated safe graft range and why?
- What is your approach to avoiding over-harvesting and patchiness?[4]
About graft survival and handling
- How are grafts stored (temperature, hydration) during the case?
- What is the typical time from extraction to implantation?
About aftercare and accountability
- What is my written aftercare plan?
- What is the follow-up schedule at 2 weeks, 3 months, 6 months, 12 months?
- What happens if growth is poor at 12–18 months?
FUE vs DHI: decision checklist (2026)
Choose based on your constraints:
- If you need a larger number of grafts, standard FUE workflows may be more efficient and easier to quality-control.
- If you need a small, precise refinement and want to minimise shaving, DHI may be worth considering.
- If the clinic’s explanation is vague, or the plan changes when you ask who does what, walk away.
A good clinic will tell you not only what they do, but what they do not do (for example, they may cap grafts per day, refuse unsafe hairline lowering, or recommend medical stabilisation first).
FAQs (search-style)
1) Is DHI better than FUE?
Not automatically. In many clinics both use FUE harvesting, and the difference is implantation workflow. Outcomes depend more on planning, donor management, graft handling, and team skill than the label.[1,4]
2) What is the difference between DHI and FUE hair transplant?
FUE describes how grafts are extracted with a small punch.[1] DHI usually describes how grafts are implanted using an implanter pen that creates the recipient site and inserts the graft.[2]
3) Is DHI more expensive than FUE in the UK?
Often yes. DHI can be slower and more staff-intensive, and pen/needle consumables add cost. But prices overlap, and surgeon involvement is usually the bigger cost driver.
4) Is DHI worth it for a no-shave hair transplant?
Sometimes. DHI is commonly marketed for no-shave or partial shave cases, but suitability depends on graft numbers, hair characteristics, and team experience. Ask the clinic to show examples of cases with similar hair length and graft counts.
5) Does DHI give higher density than FUE?
Not necessarily. “Density” depends on safe packing, blood supply, and design. Both methods can achieve strong density when done well.
6) What is Sapphire FUE and is it better?
Sapphire FUE generally means sapphire blades were used to create recipient sites.[3] It is not a guarantee of better results. Ask what problem the clinic is trying to solve by using sapphire and whether it changes your plan.
7) How long does it take to see results after FUE or DHI?
Early growth often starts around 3–6 months, with more mature results by 9–12 months. Crowns can take 12–18 months to fully mature.
8) Can FUE or DHI fail?
Yes. Poor growth can happen due to multiple factors: graft trauma, dehydration, poor planning, infection, or aggressive over-harvesting. This is why surgeon accountability and follow-up matter.[4]
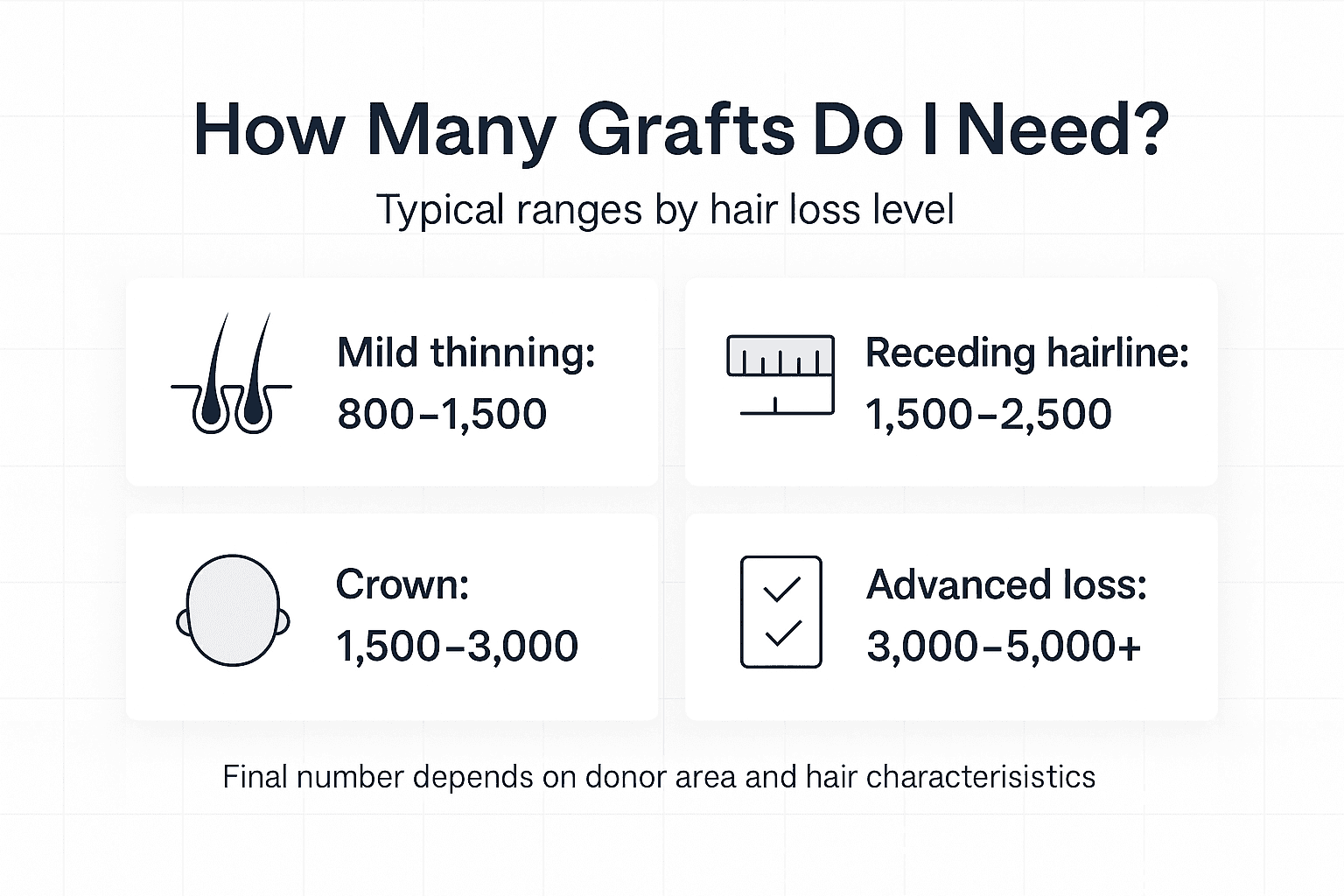
9) How many grafts do I need for my hairline?
It depends on your hair calibre, colour contrast, current miniaturisation, and how low and wide the hairline is designed. A reputable clinic will explain the reasoning rather than selling a fixed number.
Sources
- International Society of Hair Restoration Surgery (ISHRS). Follicular Unit Extraction (FUE) brings minimally invasive surgery technique to hair transplantation. https://ishrs.org/fue-minimally-invasive-technique/ (accessed 2026-02-23)
- Feller & Bloxham Medical. Should “Implanter Pens” be used during your hair transplant? https://fellermedical.com/should-implanter-pens-be-used-during-your-hair-transplant/ (accessed 2026-02-23)
- The Treatment Rooms London. Direct Hair Implantation (DHI) and implanter pen hair transplants: what you need to know. https://www.treatmentroomslondon.com/hair-transplant-tips/direct-hair-implantation-implanter-pen-hair-transplants-what-you-need-to-know/ (accessed 2026-02-23)
- Tosti A, et al. Complications in follicular unit excision hair transplantation: current evidence and practical approaches. Frontiers in Medicine. 2026. https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2026.1750989/full (accessed 2026-02-23)
Ready to Start Your Medical Journey?
Compare clinics, read verified reviews, and get personalised quotes from top medical facilities worldwide. Save up to 70% on your treatment.